18yr old male with difficulty in walking
18yr old male with complaints of "DIFFICULTY IN WALKING
I've been given this case to solve in an attempt to understand the topic of "patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with a diagnosis and treatment plan.
Following is my analysis of this patient's problem:
chief complaints of the patient.
The problems in order of priority I found are
1) difficulty in walking since 1 month
2) bilateral lower limb weakness since 1month
3)pain in lower limb calf muscles since 1 month
4)fever since 1 week
Reasons for each problem in detail.
A.Difficulty in walking and weakness of lower limbs
Onset :sudden
Duration.:since 1 month
Site:. Both legs below the knee i.e near calf
Associated complaints:
H/o difficulty in standing from sitting position.
H/o difficulty in climbing stairs
H/o difficulty in holding chappals
H/o wasting and thinning of muscles l(LL>UL)
Possible diagnosis
Difficulty in walking may be due to defect in bones,artery,muscles or nerves of that part here it is leg!
We have to rule out each and every factor.
If bone related
-Then any recent history of fracture due to trauma should be noted - in this case no
-Osteoarthritis, rhematoid arthritis can be known by xray and drug history. In this case no
We ruled out bone related cause
If Artery related
As in case of peripheral artery disease there will be pain,leg skin atrophy,and claudication. As there are no signs of this artery are ruled out.
If muscle related
if it is muscular dystrophy there should be calf muscle hypertrophy and creatine levels are Normal
Investigations-
CREATININE KINASE- 92 IU/L which is normal so muscle related cause is ruled out.
If nerves related?
May be it is related to nerves because from the history there is history of difficulty in holding chappals and wasting and thinning of muscles, difficulty in standing from sitting position, difficulty in climbing stairs.
To understand the nerve related issue
Cns examination
From the CNS examination from the case sheet
1-ANATOMICAL LOCATION OF THE PROBLEM:!
We observed that there is hypotonia,hyporeflexia,flaccid paralysis are seen a characteristic of LMN LESION(LOWER MOTOR NEURON)
Deep tendon reflexes
Right. Left
Biceps. P. ---
Triceps. ---. ---
Supinator. --- ---
Knee --- ---
Ankle. --- ---
Tone: ul. normal. Normal
LL. hypotonia. hypotonia
Power :almost all the muscles in the leg are showing 3/5 power indicating flaccid paralysis.
SPECIFIC ANATOMIC LOCATION:
Specific anatomical location should be studied to know whether the disease is from either 1)neurogenic 2)myogenic or 3) neuromuscular junction
CREATININE KINASE- 92 IU/L which is normal so muscle related cause is ruled out.
2)If suspecting Neuromuscular junction cause then electromyography should be done which is also normal in this case so it is ruled out.
3)if suspecting neurogenic cause then..
Nerve conduction studies should be done.
NERVE CONDUCTION STUDIES:


2-PHYSIOLOGICAL FUNCTIONAL DISABILTY
as there is axonal degeneration of neurons there will be functional disability of these nerves resulting in
-progressive weakness or clumsiness
-difficulty in walking
-absence of reflexes or diminished
3-ETIOPATHOLOGY
FROM the history of the patient he is alcoholic and there is anaemia. Due to alcohol consumption there is deficiency of vitamins like b1,b3,b6 which is one of the cause of peripheral neuropathy.
Calf pain is most common in ALCOHìOLIC NEUROPATHY. Due to this there will be metabolic disturbances where there is accumulation of fructose and sorbitol in Schwann cell causing axonal degradation.
https://www.slideshare.net/mobile/meducationdotnet/peripheral-neuropathy-57320857link
Other viral etiology are ruled out using investigations.
4-Other problems faced
Pain and fever
The cause of pain may be due to inflammation of these nerves and fever may be due to this inflammation of nerves.
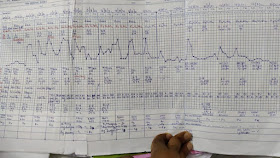
Temperature charting

Other examinations observed
On examination it came to know that he is having scabies as the lesions are present in the webspaces and on asking history he told there are same lesions in his group of members and acquired from each other.(contagious)
Diagnosis for this - scabies.
Chest x-ray and ECG are normal and thus there are no other comorbidites.
5.TREATMENT PLAN
a)pharmacological component
1-T pcm 650 mg thrice daily for fever
2-inj neomol 100ml IV infusion if fever greater than 101° f
3-T.bcomplex once daily for peripheral neuropathy
4-permethrin 5% lotion for scabies
b) non pharmacological component
Physiotherapy and proper diet sho

{kind=link}
Comments
Post a Comment